When we look at public health data through separate lenses: ageing, gender, or geography, are we compelled to notice the same profound vulnerability that occurs where they all overlap? An elderly woman living in a remote, mountainous hamlet or an isolated rural pocket does not experience these challenges as isolated data points; she experiences them simultaneously. She faces the physical vulnerabilities of advanced age, the structural socio-economic marginalization historically tied to womanhood, and the geographic isolation of an under-resourced community. In these peripheral spaces, primary health sub-centres are frequently absent or separated by significant spatial and geographic barriers that restrict physical access to care (Dang et al., 2026).
As our global population ages at an unprecedented rate: with the proportion of people over 60 projected to nearly double from 900 million in 2015 to 2 billion in 2050, ensuring access to health care for this demographic is one of the most critical public health mandates of our time (World Health Organization [WHO], 2015). To build health system, we must integrate digital health ecosystems not just for clinical efficiency, but as an act of systemic empathy. Let’s consider the global archetypes of demographic shifts; specifically, the United Kingdom, South Korea, and other international models, to understand how healthcare infrastructure can stretch to the edge.
Global Frameworks: Cross-Country Lessons in Ageing and Isolation
To build an equitable roadmap, we must evaluate how hyper-aged or rapidly transitionary societies handle health access at the periphery:
Country
Core Demographic Challenge
Institutional Response
The Digital Integration
International Model
Super-aged Society: Over 29% of the population is 65 or older. Severe rural depopulation has left elderly women isolated in dying, edge-case villages.
Integrated Community Care System: Focuses heavily on housing, healthcare, and long-term preventive care within a strict 30-minute living radius.
High reliance on automated home monitors, remote tracking of vital parameters, and community-level digital check-ins to counter lonely deaths.
South Korea
Fastest-ageing Developed Nation: Faced with a steep demographic cliff and a high elder poverty rate, heavily concentrated among older women.
Community-based Integrated Care: Decentralizing specialized geriatric clinical care directly to local rural townships and community hubs.
"Smart Care" initiatives utilizing tablet-based health tracking managed by visiting nurses, paired with AI voice-assistants for mental health tracking.
United Kingdom
The Loneliness Epidemic: Geographic isolation in coastal and rural shires, with older women disproportionately living alone with multiple chronic conditions (multimorbidity).
NHS Long Term Plan & Social Prescribing: Empowering general practitioners (GPs) to connect isolated individuals to community-based support groups instead of purely medical solutions.
The NHS App ecosystem integrated with virtual wards, allowing complex chronic disease management to happen safely inside rural homes.
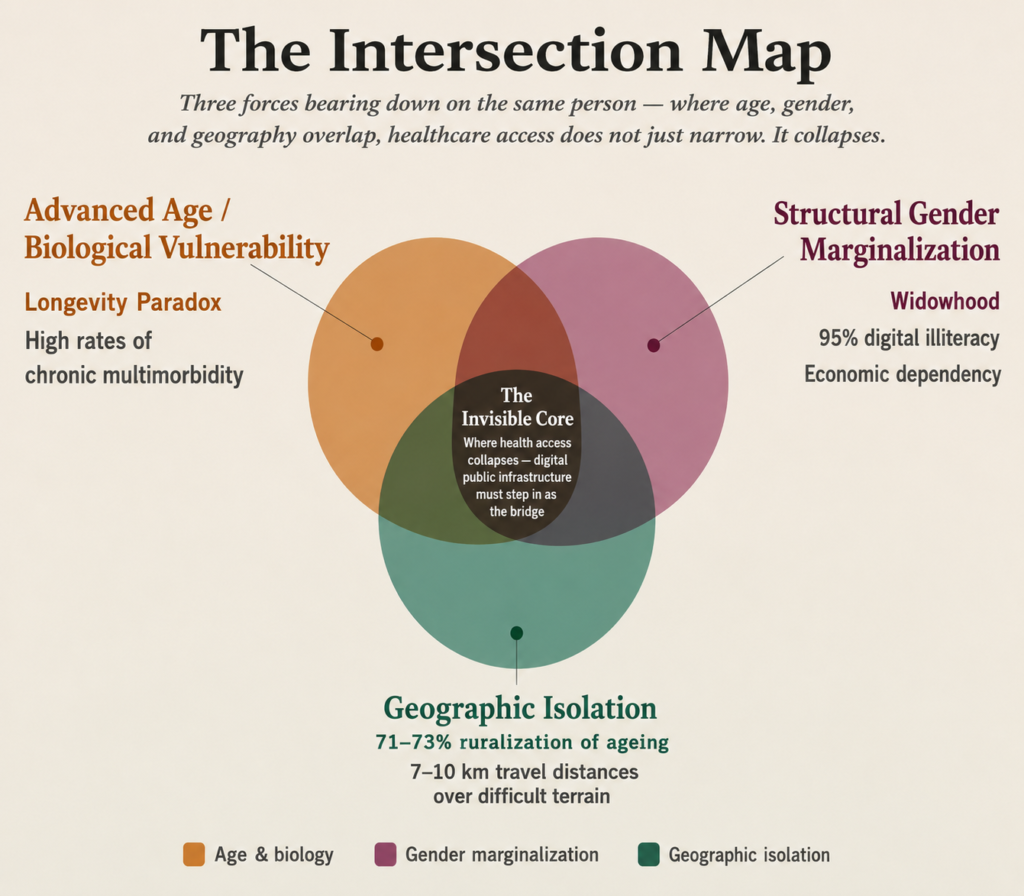
The Common Link: The Intersectional Vulnerability of Older Women
Why do women bear the heaviest burden within remote, ageing populations? The answer lies in the life course approach to public health, where advanced age converges with structural gender marginalization, financial dependence and geographic isolation. This creates a complex web of vulnerability that manifests across three distinct dimensions:
The Longevity Paradox: Across almost all societies, women have a higher life expectancy than men, but they often spend those additional years facing higher rates of chronic disability and illness (WHO, 2015). Because they outlive their spouses, a high proportion of older women end up living entirely alone in remote areas, stripped of immediate domestic support structures.
Economic and Social Dependency: Due to historical gaps in formal workforce participation, older women in rural communities are significantly less likely to have independent pensions, land ownership or financial reserves. This financial dependence transforms seeking healthcare from an individual choice into a complex family negotiation, where the woman’s health needs are frequently deprioritized (LASI Wave 1, 2017–18 report)
The Tyranny of Distance: In remote communities, reaching a secondary or tertiary healthcare facility requires a gruelling journey across difficult terrain. For an elderly woman suffering from osteoarthritis, visual impairment, or frailty, a long travel distance isn’t just an inconvenience; it is a physical impossibility. (Dang et al., 2026)
When physical barriers, financial dependence, and geographic isolation converge, traditional healthcare access completely collapses. This is where digital health must step in, not as a luxury, but as a bridge.
Reimagining India’s Digital Public Infrastructure (DPI) with Empathy
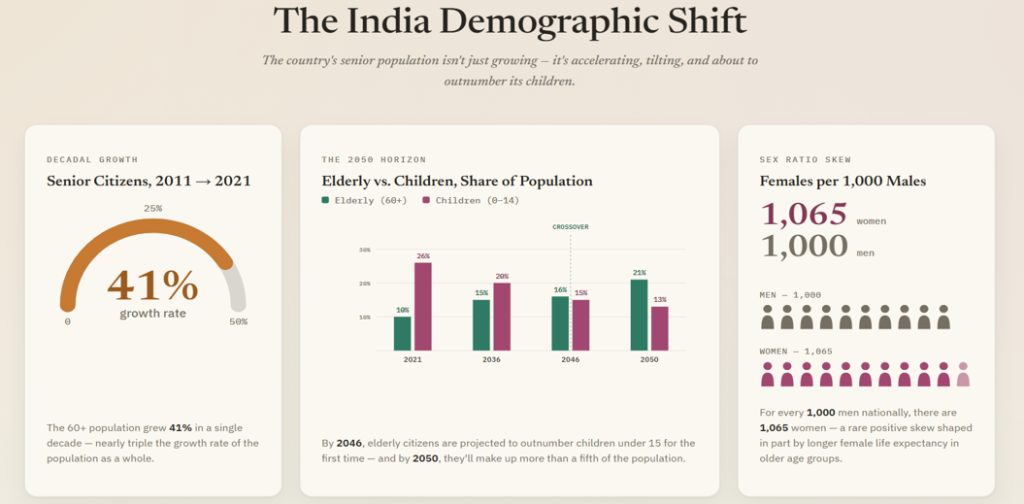
While global archetypes offer vital structural frameworks, translating these lessons to the Indian context requires confronting a demographic reality and geographic differentiation of staggering proportions. India is experiencing an unprecedented demographic transition. According to the United Nations Population Fund (UNFPA) India Ageing Report 2023, the country’s elderly population (aged 60 and above) is growing at a decadal rate of 41%. It is projected to double to over 20% of the total population by 2050, surpassing the population of children under 15 by 2046 (UNFPA, 2023). Crucially, this expanding demographic is defined by two unique phenomena:
The Ruralisation of Ageing: An overwhelming 71%-73% of India’s senior citizens reside in rural pockets. This creates an intense geographical imbalance where expanding geriatric healthcare demands are concentrated in areas least equipped with physical medical infrastructure.
The Feminisation of Ageing: Driven by higher life expectancy at older ages, the elderly sex ratio heavily skews toward women, reaching an average of 1,065 females per 1,000 males nationally. This escalates to even higher concentrations of highly vulnerable, single older women in remote settings (UNFPA, 2023).
Real-World Bottlenecks: India’s Core Public Health Challenges
To design an effective digital lifeline, we must first acknowledge the multi-layered structural challenges that an isolated elderly Indian woman faces:
The Intersection of Widowhood and Poverty: According to the UNFPA India Ageing Report 2023, over 54% of elderly women in India outlive their partners, facing a severe “feminisation of poverty“. This high prevalence of widowhood directly triggers structural vulnerability; lacking formal income security, personal assets, or independent land ownership, more than 40% of India’s elderly find themselves in the poorest wealth quintile. Consequently, without personal financial autonomy, seeking clinical healthcare is rarely an independent choice: it is an unaffordable event that often results in high out-of-pocket health expenditures for the household.
The Double Barrier of Literacy: While legacy health systems rely heavily on patient self-reporting, older rural women experience profound systemic marginalization. According to the LASI Wave 1, 2017–18 report, only around 31% of women aged 60-75 are literate. More critically, it reveals that 95% of elderly women in India are digitally illiterate.
The Burden of Multimorbidity:LASI Wave 1 data points out that nearly 45% of India’s overall disease burden will be driven by older adults by 2030, heavily dominated by chronic conditions like cardiovascular diseases, hypertension, diabetes, and depressive symptoms.
Empowered Solutions: Blueprint for the Margins
India possesses a world-class digital health framework through the Ayushman Bharat Digital Mission (ABDM) and the eSanjeevani telemedicine grid. To bridge the massive digital divide, our public health strategy must wrap this digital architecture in a concise, human-centric framework:
“Phygital” Health Pathways: Equipping ASHAs and ANMs with point-of-care diagnostic tablets transforms routine home visits into mobile clinical hubs. Frontline workers can capture vitals, link them directly to the patient’s Ayushman Bharat Health Account (ABHA), and use eSanjeevani to patch in urban specialists directly to the remote bedside. (Szczepura et al., 2023)
Longitudinal Care Registries: Digitizing non-communicable disease (NCD) trends, pharmaceutical dependencies, and clinical history ensures safe, error-free longitudinal treatment, even when elderly patients migrate between different rural families. (UNFPA, 2023, Szczepura et al., 2023)
Data-Driven Doorstep Delivery: Instead of forcing frail individuals onto gruelling journeys for basic care, public health networks must use targeted community outreach and the doorstep delivery of monthly chronic maintenance medications to close physical gaps in health opportunity (LASI Wave 1, 2017–18 report, Jia et al., 2024)
Conclusion: The Ultimate Test of Public Health Equity
The true measure of a nation’s public health ecosystem is not how seamlessly it operates within its high-tech urban centres, but how effectively it shields its most vulnerable, silent individual at the farthest periphery. By combining the structural community integration of international models, the data-driven precision of South Korea, and the human-centric focus of the UK with India’s powerful Digital Public Infrastructure, we can create an indigenous healthcare model that leads with dignity. Digital health transformation is ultimately not a story about software, cloud registries, or servers. It is a story about visibility and inclusivity. It is about ensuring that an older woman, sitting in a remote home, hours away from the nearest city, is seen, valued, and instantly connected to the care she fundamentally deserves.
References
Jia J, Jia C, Zhang X, Ren P, Chen M, Xu J. (2024). The Impact of Internet Medical Service on Rural Gender Inequality in Health Opportunity: A Cross-Sectional Study.BMC Public Health, 24(1), 3093. https://doi.org/10.1186/s12889-024-20575-w
Dang, A., Ratra, V., Singh, D., & Gupta, I. (2026). Granular evaluation of public primary healthcare accessibility in rural India. LSE Research Online Documents on Economics 138085, London School of Economics and Political Science, LSE Library.
Szczepura A, Masaki H, Wild D, Nomura T, Collinson M, Kneafsey R. (2023). Integrated Long-Term Care ‘Neighbourhoods’ to Support Older Populations: Evolving Strategies in Japan and England. International Journal of Environmental Research and Public Health, 20(14), 6352. https://doi.org/10.3390/
International Institute for Population Sciences (IIPS), National Programme for Health Care of Elderly (NPHCE), Ministry of Health and Family Welfare (MoHFW), Harvard T.H. Chan School of Public Health (HSPH), & University of Southern California (USC). (2020). Longitudinal Ageing Study in India (LASI) Wave 1, 2017–18: India Report. Mumbai: International Institute for Population Sciences.
International Institute for Population Sciences (IIPS) & United Nations Population Fund (UNFPA). (2023). India Ageing Report 2023: Caring for Our Elders – Institutional Responses. New Delhi: United Nations Population Fund.
World Health Organization. (2015). World report on ageing and health. World Health Organization.
United Nations, Department of Economic and Social Affairs, Population Division. (2022). World Population Prospects 2022: Summary of Results. New York: United Nations. Available at: World Population Prospects 2022: Summary of Results
Raania Gautam is a postgraduate Public Health student at Dr B.R. Ambedkar University, Delhi, driven by a commitment to bridging gaps in community health systems. Transitioning from life sciences to institutional advocacy, her research focuses on bringing dignity to primary healthcare infrastructure and addressing intersectional vulnerabilities among marginalized populations. As Sankala Foundation’s first Public Health intern, she channels her academic pursuit into policy analysis, data modeling, and mapping the linkages between climate change and constitutional rights. She believes that impactful advocacy requires both structural precision and a compassionate approach to systemic equity.