Beyond Apps: The Transformative Power of Digital Health on the Ground
Dr Simran Dutta
Digital health is often imagined as mobile applications, online consultations, or dashboards. But on the
ground, it is much more than technology, it is about making healthcare systems more connected,
coordinated, and human centred.
For many people living in rural India, accessing healthcare is not simply about reaching a hospital. It is about
knowing where to go, whether a doctor will be available, how long the wait will be, and whether the visit will
mean losing an entire day’s wages.
Over the past three decades, India’s healthcare system has made significant progress in improving health
outcomes, expanding healthcare infrastructure, and strengthening service delivery mechanisms. Yet, despite
these achievements, ensuring equitable access to healthcare for underserved populations, particularly those
living in rural and remote geographies, continues to remain a challenge.
Video consultation in a V-POD room at a DiNC-enabled health facility in Kolar district, Karnataka
National Goals in Health: Universal Health Coverage
The COVID-19 pandemic marked a significant turning point in the integration of digital technologies into
India’s healthcare system. As movement restrictions and concerns about infection limited access to in-person
healthcare services, telemedicine platforms such as eSanjeevani emerged as vital tools for ensuring
continuity of care. The platform enabled citizens to consult healthcare professionals remotely, improving
access to medical services from the safety and convenience of their homes. Its rapid expansion during and
after the pandemic highlights the growing role of digital health in advancing Universal Health Coverage (UHC)
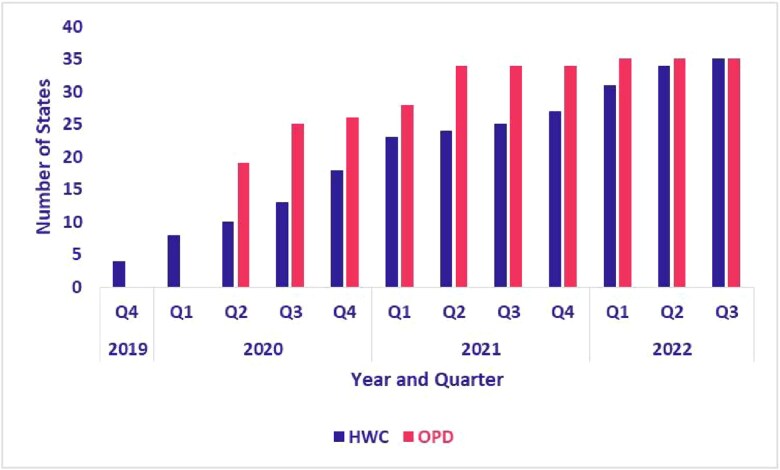
in India. As noted by Sood et al. (2025), the rapid expansion of eSanjeevani reflects the successful scale-up
of a government-led telemedicine platform integrated into India’s public health system. This trend is evident
in Fig. 1, which shows the steady increase in the number of States and Union Territories adopting eSanjeevani
services through Ayushman Bharat Health and Wellness Centres (AB-HWCs) and OPD services between 2019
and 2022.
By February 2023, the platform had already served more than 10 crore people demonstrating the immense
potential of digital health in improving healthcare accessibility across the country. Of the total beneficiaries,
57% were women and 12% were senior citizens. This shows the innovation’s ability to reach not just rural
and remote areas, but also the most vulnerable groups of the society (PIB, 2023).
Fig.1: Adoption of eSanjeevani AB-HWC and OPD by states and UTs (Source: Sood et al., 2025)
What does digital health look like on the ground?
To better understand this question, Sankala Foundation undertook a study of the DiNC (Digital Nerve Centre) model implemented in Kolar district, Karnataka.
A 32 seater Digital Nerve Center Located within the premises of the DHO officer, Kolar
To streamline processes in public health facilities, reduce patient overload in secondary and tertiary hospitals,
and increase the utilisation of Primary Health Centres (PHCs), healthcare model was introduced which
leveraged the use of technology in bringing primary care close to the rural communities in Kolar district. This
model was developed in partnership with Tata Medical and Diagnostics (Tata MD) and the Department of
Health and Family Welfare (DoHFW- GoK).
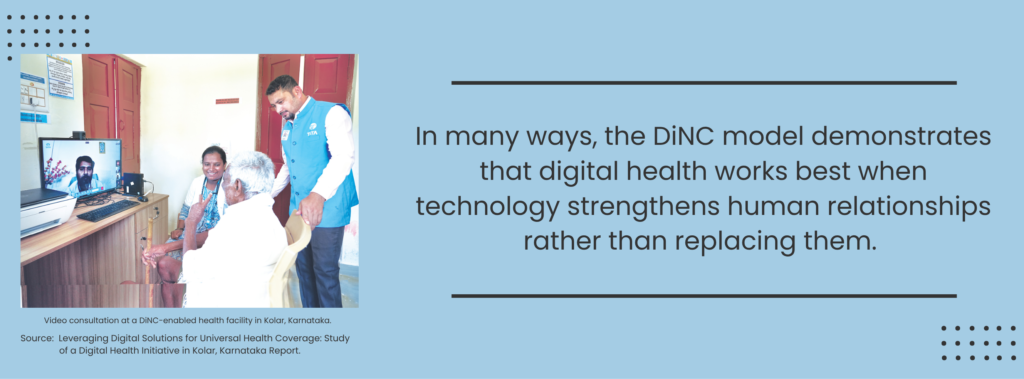
What makes the initiative particularly interesting is that it does not rely on technology alone. At the centre
of the system are Patient Care Coordinators (PCCs), who act as a bridge between healthcare providers and
patients. These coordinators help patients navigate appointments, understand prescriptions, receive
reminders for follow-up care, and access specialist consultations when needed. In many ways, the DiNC
model demonstrates that digital health works best when technology strengthens human relationships rather
than replacing them.
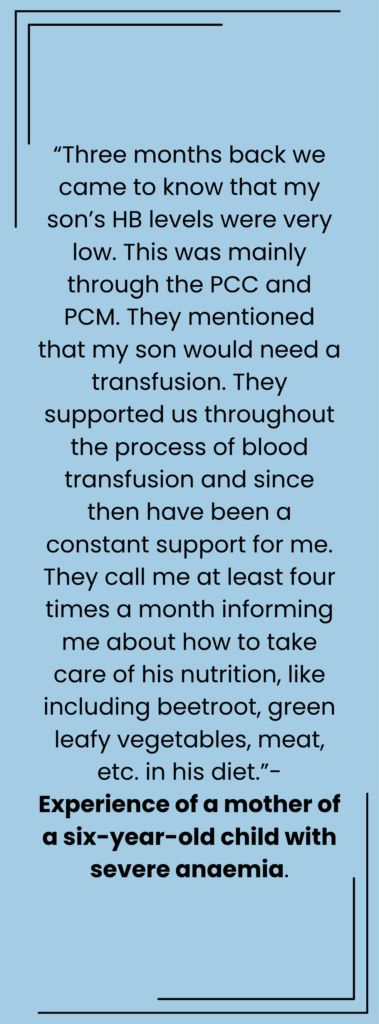
The impact of this approach becomes more visible through the experiences shared by mention the healthcare workers and patients themselves.
One tuberculosis patient described how regular follow-up calls and counselling support helped ensure adherence to medication:
“Eight months back, I was diagnosed with TB and successfully got cured two
months ago. Adhering to the daily medication was not easy… I developed a
lot of stomach issues… but support from Salma (PCC) and regular calls from
the centre nurses proved very helpful. They emphasised the importance of
not skipping the medication and offered tips for maintaining good nutrition
and exercise, mainly walking. They also informed us about the ₹500/ month
benefit for TB patients. I also received a monthly nutrition package
containing jaggery, lentils and groundnuts.
What has changed? Access to relevant information as explained by a Patient Care Co-ordinator:
“As the PHCs in Kolar are networked under DiNC, if a primary
health centre doctor feels that the patient requires a
specialist opinion, the patient is referred to the higher
centres and the concerned specialist. In this way, the
patient has better access to treatment and is less likely to visit a quack. An important
factor is follow-up. The DiNC has details of all the patients that I treat in a day… So,
it’s good for us and it has increased the doctor-patient time interaction. The time
taken for diagnosis also gets reduced.”
An NCD patient from Kolar city, who has been undergoing treatment for diabetes and hypertension for the past four years, became aware of the DiNC initiative two years ago and subsequently reported a reduction in out-of-pocket expenditure due to access to free medications provided through government health facilities:
“Earlier I used to go to a private hospital where I was spending at least ₹200 to ₹300
per consultation and additional expenditure for medications. After I started visiting
the government facility, I did not incur any expenditure… I got the medication required
for one month free of cost. I get a refill whenever it is over.”
Patient Care Coordinator assisting patients at a health facility
PCCs seen assisting patients at the DiNC micro-arena, SNR District Hospital
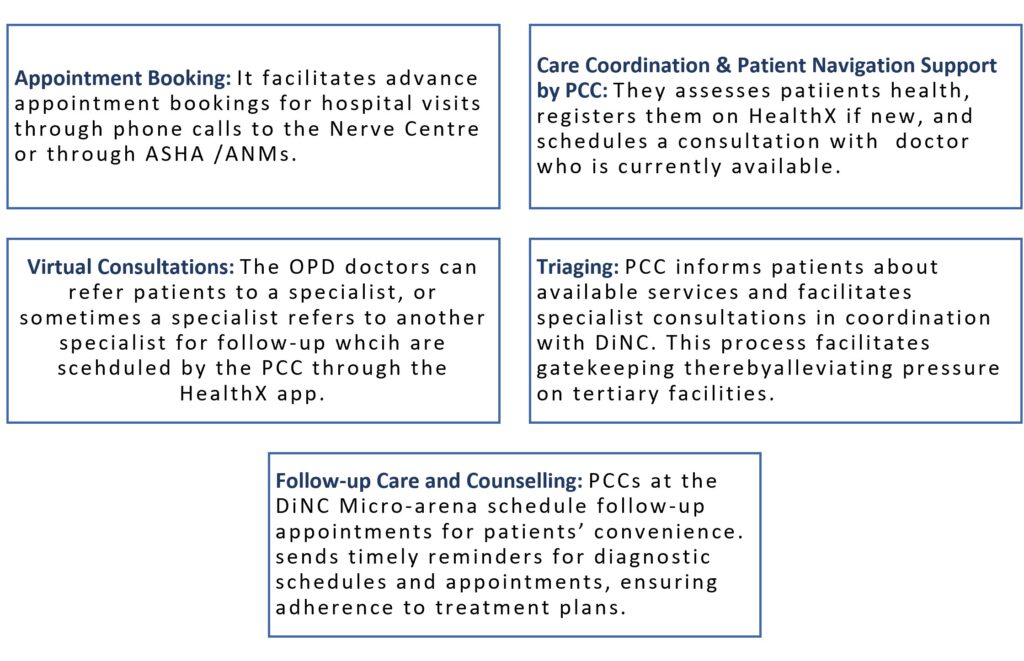
The core activities in the DiNC model and highlighted below
Impact of the DiNC Model
Patient Registration: With the involvement of ASHA workers, within 5 months of the inception of the model in 2017, there was a significant upsurge in patient registration. A slight peak was observed during 2021 due to the COVID pandemic. A total of 1,00,091 female registrations were reported in 2022–2023, compared to 86,465 male registrations.
Video Consultations: There was a steady rise in this domain as well, with over 18,000 consultations conducted in 2022–23 alone, most of them for Lamaze sessions.
Immunization Coverage: The DiNC has facilitated the immunization of more than 50,000 children in 2022–23, which is a remarkable achievement.
Conclusion
Initiatives like DiNC have quietly transformed the everyday healthcare experiences of people living in Kolar district. For many residents, the initiative meant shorter journeys to hospitals, easier access to doctors, timely follow-ups, free medicines, and most importantly, the reassurance that someone within the system was consistently guiding and supporting them through their care journey.
At its core, the DiNC model tells a larger story about what digital health can achieve when technology is combined with human-centred care. It highlights how effective collaboration between the government and private sector can create innovative and scalable solutions capable of strengthening healthcare access for communities that are often left behind.
Its true value lies in making healthcare systems feel more connected, responsive, and compassionate for people who struggle the most to access timely care.
References:
Press Information Bureau. (2023, February). Union Health Minister, Dr Mansukh Mandaviya hails the “eSanjeevani” landmark milestone of providing telemedicine services to more than 10 crore patients. Ministry of Health and Family Welfare, Government of India. https://pib.gov.in/PressReleasePage.aspx?PRID=1899855
This blog is based on the report, Leveraging Digital Solutions for Universal Health Coverage: Study of a Digital Health Initiative in Kolar, Karnataka.
All images featured in this blog are sourced from the original report.
Dr Simran Dutta is a public health professional specialising in digital health, health systems strengthening, and research. She holds a degree in Homoeopathic Medicine and a PGDM in Health Management from IIHMR, New Delhi. At Sankala Foundation, she contributes to research, policy analysis, and technology enabled solutions to improve healthcare access and outcomes.